

Starlight Adolescent Center Program Overview
Stars(BeHaviorafJSeaCtfi (^roup
Starlight Adolescent Center
OVRRVIEW OF PROGRAM
(Hienrs Served July 2003 through Dec 2004
Mission
Starlight Adolescent Center expresses the clisrincdvc mission and ^dsion of residential and
commuiiiiy outpatient treatment within the larger mission of Stars Bebamral Health Croup(SBHG);
“Develop and operate a full continuu/n of mental health sendees that leflect clinical excellence and continuous cjuality
improvements, to maintain an unconditional commitment to assisting clients ndth mental illness to achieve and maintain
their optimum level offunctioning and quality of life, and to proidde effective mental health treatment and cost-efficient
sendees that involve and respect the diverse resources and talents available ndthin the client,jamily, sfaj], and community”.
Witliin the SBMG continuum, Starlight Adolescent Center has the important distinction of offering
to (California the first(Communirv Treatment Facility (CTF)for youth. Started in year 2000, the original
CCTF mission was to provide local and cost-effective tteatment as an alternative to expensive state
hospitalization. This mission was accomplished as state hospital populations declined and youtli moved
into community care, Subsequently, Starlight began to play a unique role in the continuum of services
available throughout the state by providing a step-up for clients unable to succeed witliin an RCI.J.cvel
12-14 group home. CTFs also offer treatment- as distinct from detention — to juvenile offenders with
mental illness. Starlight’s (I'i’F
and Non-Public School(NFS)
make step-down and sustained
safety, stmeture, treatment, and
education possible for youth
coming from acute or sub-acute
psychiatric facilities.
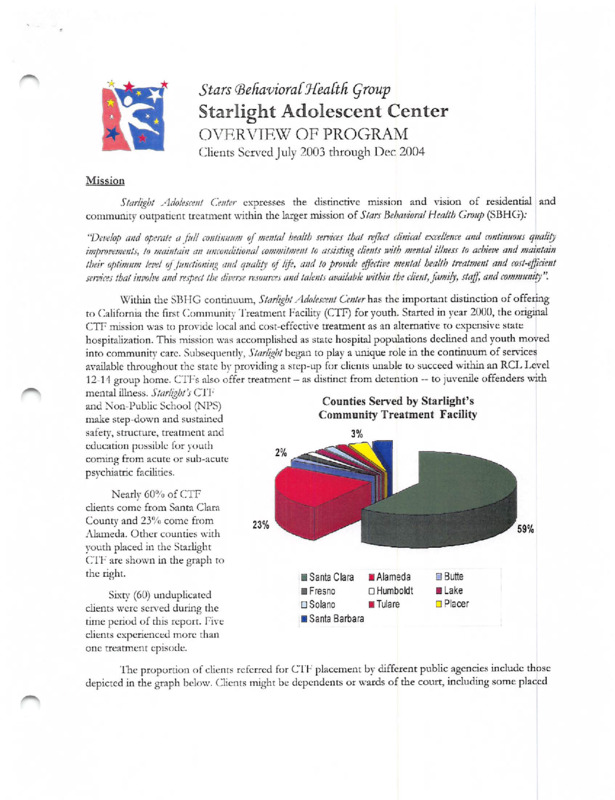
Counties Served by Starlight’s
Community Treatment Facility
2%
r .
Nearly 60% of CTF
clients come from Santa Cilara
(iounty and 23‘Fo come from
23%
Alameda. CJther counties with
youth placed in the Starlight
CTF' are shown in the graph to
the right.
Sixr\- (60) unduplicated
clients were sciv'ed during the
rime period of this report. Five
clients experienced more than
one treatment episode.
S Butte
i Santa Clara
lAlameda
a Fresno
□ Humboldt
■ Lake
□ Solano
■ Tulare
□ Placer
■ Santa Barbara
The proportion of clients referred for CT'F placement by different public agencies include those
depicted in the graph below. Clients might be dependents or wards of the court, including some placed
voluntarily as an alternative to
detention. Upon referral, potential
Referring Agencies
CTF clients are assessed and
authorized for placement through the
Santa Clara County Mental Health
Department.
More recently. Starlight Community
■ Probation ■ Social Services □ MH Special Education
Services has begun to offer intensive day
treatment, non-public schooling,
specialty outpatient mental health
sendees, and therapeutic behavioral
sendees to community chents in order
to prevent the need for higher level
placements or hospitalizations in the
first place.
Client and Family Outcomes fProgram Goalsi
The outcomes we work tenvard with youth and families arc that y^outh be:
'’‘It Safe in home err family’ like settings -- including avoiding out-of-home placements, returning to lower
levels of care, fostermg pennanency, and positively impacting family functioning;
'•k Attending and progressing in school or vocational endeavors — including improving
school/vocational attendance and engagement, improving grades and grade-level advancement.
and enhancing standardized achievement test scores;
-•k Improved health/mental health functioning - including improving access to needed health/mental
health care, improved functioning in multiple life domains, reduced psychiatric risk (risk factors
and risk behaviors), and builchng community’ supports; and,
including reducing arrests, criminal detentions, and probation
■•k Out of trouble with the law
involvement.
CTF Youth Demographic Profile
Starlight Adolescent Center ser\’es adolescents of both genders that come from a variety of
backgrounds. Over the time period covered in this report, youth were 5.3% male and 47% female.
Age at Admission of Starlight CTF Clients
30%
25%
Starlight youth are ages 12 through
17 upon admission. The average
age is 15 and 50% arc age 15 or
younger.
20%
15%
10%
5%
0%
12Yrs
I
13Yrs
Starlight Summar)- of Program
I I
14 Yrs
15 Yrs
16Yrs
Chents are in treatment at Starlight
from less than one month up to
,38 months. The average length of
stay is 11.9 months (just under a
year).
17 Yrs
KLD V.0.VO6/05
2 of 5
'iTic ethnicities of clients arc:
Ethnicity of Starlight CTF Clients
Native
Other
African
41% European anccstr}', 29%
Latino, 22% African iVmerican,
1.2%
American
6% Asian(3% Vietnamese,3%
American
Latino
Other Asian), and 1% each Native
21.7%
American and Other/Unknown.
1.2%
All Asian
28.9%
Starlight's demographic data
6.0%
show an increase in Asian youth
X'
European
41.0%
served in h’Y 03-04 compared to
the prior year (from 1% to 6%
combined,3% being Vietnamese).
This is consistent with the shifting
demographics of Santa Elara
County, which now reports 4
threshold language groups
(Spanish, Mandarin,I’agalog and
Vietnamese).
CTF Youth Clinical Profile
The youth sensed in the Starlight Community Treatment Tacility(CTF)suffer from severe emotional
dismrbancc and must meet medical necessity criteria for enrollment in a structured treatment
environment. The youth entering the CT b residential program have a history of troubled behavior
including aggressive, oppositional, provocative, impulsive, and self-destmctivc behaviors, often
accompanied by intense negativism and social withdrawal. Along with these behaetiors, the youth
t\rpically suffer from strained or impaired interpersonal and family relationships, resulting in an absence
of vital social support.
The residential youngsters have experienced one or more treatment failures in outpatient,
extended care management,or less restrictive settings. If not in the stable and intensive treatment
environment of the StarlightCTSl', the youth would be in psychiatric hospitals, or continue to move
among placements, treatment
1
Prior Service History
settings, shelters, and juvenile
Average
IXPe
detention. Their behavior may
3.6
represent a potential danger to
; Psychiatric Hospitalizations
4.1
self, others and/or property, and j Group Home Placements
their treatment requires
1.0
: Foster Family Placements
comprehensive evaluation,
.3
: Shelters
close staff supcnnsion, intensive
8.7
, Combined Prior Placements
therapy, remedial education, and
monitoring of the need for pharmacotherapy.
Range
Oto 15
Oto 21
Oto 10
Oto 3
1 to 28
The psychiatric problems of the C'i'T youth include both internalizing (e.g., anxiety, depression
and self-harm behavior) and externalizing (e.g., attentional, impulsive and aggressive behaviors)
problems. Many clients exhibit a combmation of disorders across these broad spectmms. On average,
CTF clients have two major diagnoses (on Axis 1 of the DSM IV)and many of the diagnoses are
characterized bv complicating feamres (e.g., psychotic features associated with a diagnosis of Bipolar
Disorder).
I
The combined figure is an undercount, as counts of prior juvenile detentions are not currently available.
Starlight Summarj- of Program
KLD v.().5/06/05
3 of 5
Types of Disorders (Percent Clients with a Diagnoses)
Most Prevalent Diagnoses
100
90
80
68%
60%
70
Bipolar Disorder
30%
Post Traumatic Stress
29%
Other Mood Disorders
25%
Major Depression
23%
60
50
40
30
12%
20
Att-Def Hyperactivity
22%
Conduct Disorder
19%
Oppositional Defiant
15%
Intermittent Explosive
13%
10
0
Internalizing
Externalizing
Other
Disorders
Disorders
Disorders
Schizoaffective
9%
Schizophrenia
3%
As can be seen in the graph below, Starlight clients have DSM Axis V Global^Assessment of
\hmctionmg(GAP)scores ranging frem 20 to 62 on a 0 to 100 point rating scale, where 100 is optimal
functioning. Tire average GAF score is 36.4, median is 35.0, and the standard deviadon is 8.75 (modest
amount of variadon in physician’s ratings of funedoning).'i'wenty-five percent(25%) of clients have a
GAF score of below 30 upon enrollment.
100
Interpreting GAF Scores
51-60: Reflects moderate difficulties in social or school
funedoning with symptoms not apparent at aU times
or in all areas.
High = 62
Average = 36.4
Low = 20
0
41 -50: Reflects serious impairments in social or school
functioning (e.g., frequent aggressive or antisocial
behavior, suicidal preoccupation).
31-40: Reflects major impairments in several areas
(e.g., persistent aggression without clear
instigation, markedly withdrawn and isolated,
suicide attempts).
Below 30: Serious impairment in almost aU areas (e.g.,
stays in bed all day, severe impairment in reality
testing, communications sometimes incoherent).
Youth Outcomes
Hffecting outreach, family building, and transition planning is always challenging with a high-end
sendee population. Many families are ill-equipped and need much help to receive and maintain troubled
youth in the home. Poor and mentally disturbed young adults struggle with a shortage of safe, low-cost
housing in the Bay Area. Fiducaticmal options are often limited and ongoing support may be needed to
help youth stay focused and on track with educational or vocational endeavors. Cultural competency
implies wc help youth and families with these kinds of everyday life challenges. For all of the above
reasons, permanency or emancipation planning is a major focus of Starlight staff attention and effort.
Starlight Sumniar\- of Program
K1.D v.05/06/05
4of5
One measure of mental health
Increase in Functioning
funcaoning is the change in CjAF
100
scores from admission to
90
discharge. On average, the CrF
youth show a 5.14 gain in their
rating, which is statistically
significant (p <.005)improvement
of modest si2e (that is, clients
move up one scale level on the
description of the GAF found on
the previous page).
80
70
60
50
41.5
36.4
40
30
20
10
0
GAF at Placement
GAF at Discharge
/Vnothcr indicator of
treatment impact is tlic
ability of clients to
transition to a lower level
Placement at Discharge(As Percent of All Discharged Clients)
60.0%
of care. As can be seen
from the chart at right,
over half of youth (64.5%)
are able to step-down to
their family home, foster
family, or a lower level
group home.
Along with the
increasing numbers of
youth admitted from
juvenile probation, we have
48.4%
50.0%
40.0%
29.0%
30.0%
20.0%
16.1%
10.0%
6.5%
seen an increase in
0.0%
discharges back to juvenile
Hospital/Adult
Juvenile Hall
Home/Family
Group Home
hall, usually related to
IMD
significant violence and
aggression. Currently, we
are meeting tins challenge by implementing a restoradve jusdee component to the treatment program.
In summaty^, Starlight remains an intensive, muldfaceted community mental healdr treatment
program for die most seriously emotionally dismrbed youth in California. The program is effeedve in
stabihzing and reuniting youth with their families in shorter periods of dme and with greater frequency
than other previous mental health and social sendee programs. Tlnough the Starlight Community Services
program, Starlight is able to ensure condnued stabiHzadon of these youth in their homes,school and
communit^^
Starlight Summary- of Program
Kl.D v.05/06/().5
5 of5
Starlight Adolescent Center
OVRRVIEW OF PROGRAM
(Hienrs Served July 2003 through Dec 2004
Mission
Starlight Adolescent Center expresses the clisrincdvc mission and ^dsion of residential and
commuiiiiy outpatient treatment within the larger mission of Stars Bebamral Health Croup(SBHG);
“Develop and operate a full continuu/n of mental health sendees that leflect clinical excellence and continuous cjuality
improvements, to maintain an unconditional commitment to assisting clients ndth mental illness to achieve and maintain
their optimum level offunctioning and quality of life, and to proidde effective mental health treatment and cost-efficient
sendees that involve and respect the diverse resources and talents available ndthin the client,jamily, sfaj], and community”.
Witliin the SBMG continuum, Starlight Adolescent Center has the important distinction of offering
to (California the first(Communirv Treatment Facility (CTF)for youth. Started in year 2000, the original
CCTF mission was to provide local and cost-effective tteatment as an alternative to expensive state
hospitalization. This mission was accomplished as state hospital populations declined and youtli moved
into community care, Subsequently, Starlight began to play a unique role in the continuum of services
available throughout the state by providing a step-up for clients unable to succeed witliin an RCI.J.cvel
12-14 group home. CTFs also offer treatment- as distinct from detention — to juvenile offenders with
mental illness. Starlight’s (I'i’F
and Non-Public School(NFS)
make step-down and sustained
safety, stmeture, treatment, and
education possible for youth
coming from acute or sub-acute
psychiatric facilities.
Counties Served by Starlight’s
Community Treatment Facility
2%
r .
Nearly 60% of CTF
clients come from Santa Cilara
(iounty and 23‘Fo come from
23%
Alameda. CJther counties with
youth placed in the Starlight
CTF' are shown in the graph to
the right.
Sixr\- (60) unduplicated
clients were sciv'ed during the
rime period of this report. Five
clients experienced more than
one treatment episode.
S Butte
i Santa Clara
lAlameda
a Fresno
□ Humboldt
■ Lake
□ Solano
■ Tulare
□ Placer
■ Santa Barbara
The proportion of clients referred for CT'F placement by different public agencies include those
depicted in the graph below. Clients might be dependents or wards of the court, including some placed
voluntarily as an alternative to
detention. Upon referral, potential
Referring Agencies
CTF clients are assessed and
authorized for placement through the
Santa Clara County Mental Health
Department.
More recently. Starlight Community
■ Probation ■ Social Services □ MH Special Education
Services has begun to offer intensive day
treatment, non-public schooling,
specialty outpatient mental health
sendees, and therapeutic behavioral
sendees to community chents in order
to prevent the need for higher level
placements or hospitalizations in the
first place.
Client and Family Outcomes fProgram Goalsi
The outcomes we work tenvard with youth and families arc that y^outh be:
'’‘It Safe in home err family’ like settings -- including avoiding out-of-home placements, returning to lower
levels of care, fostermg pennanency, and positively impacting family functioning;
'•k Attending and progressing in school or vocational endeavors — including improving
school/vocational attendance and engagement, improving grades and grade-level advancement.
and enhancing standardized achievement test scores;
-•k Improved health/mental health functioning - including improving access to needed health/mental
health care, improved functioning in multiple life domains, reduced psychiatric risk (risk factors
and risk behaviors), and builchng community’ supports; and,
including reducing arrests, criminal detentions, and probation
■•k Out of trouble with the law
involvement.
CTF Youth Demographic Profile
Starlight Adolescent Center ser\’es adolescents of both genders that come from a variety of
backgrounds. Over the time period covered in this report, youth were 5.3% male and 47% female.
Age at Admission of Starlight CTF Clients
30%
25%
Starlight youth are ages 12 through
17 upon admission. The average
age is 15 and 50% arc age 15 or
younger.
20%
15%
10%
5%
0%
12Yrs
I
13Yrs
Starlight Summar)- of Program
I I
14 Yrs
15 Yrs
16Yrs
Chents are in treatment at Starlight
from less than one month up to
,38 months. The average length of
stay is 11.9 months (just under a
year).
17 Yrs
KLD V.0.VO6/05
2 of 5
'iTic ethnicities of clients arc:
Ethnicity of Starlight CTF Clients
Native
Other
African
41% European anccstr}', 29%
Latino, 22% African iVmerican,
1.2%
American
6% Asian(3% Vietnamese,3%
American
Latino
Other Asian), and 1% each Native
21.7%
American and Other/Unknown.
1.2%
All Asian
28.9%
Starlight's demographic data
6.0%
show an increase in Asian youth
X'
European
41.0%
served in h’Y 03-04 compared to
the prior year (from 1% to 6%
combined,3% being Vietnamese).
This is consistent with the shifting
demographics of Santa Elara
County, which now reports 4
threshold language groups
(Spanish, Mandarin,I’agalog and
Vietnamese).
CTF Youth Clinical Profile
The youth sensed in the Starlight Community Treatment Tacility(CTF)suffer from severe emotional
dismrbancc and must meet medical necessity criteria for enrollment in a structured treatment
environment. The youth entering the CT b residential program have a history of troubled behavior
including aggressive, oppositional, provocative, impulsive, and self-destmctivc behaviors, often
accompanied by intense negativism and social withdrawal. Along with these behaetiors, the youth
t\rpically suffer from strained or impaired interpersonal and family relationships, resulting in an absence
of vital social support.
The residential youngsters have experienced one or more treatment failures in outpatient,
extended care management,or less restrictive settings. If not in the stable and intensive treatment
environment of the StarlightCTSl', the youth would be in psychiatric hospitals, or continue to move
among placements, treatment
1
Prior Service History
settings, shelters, and juvenile
Average
IXPe
detention. Their behavior may
3.6
represent a potential danger to
; Psychiatric Hospitalizations
4.1
self, others and/or property, and j Group Home Placements
their treatment requires
1.0
: Foster Family Placements
comprehensive evaluation,
.3
: Shelters
close staff supcnnsion, intensive
8.7
, Combined Prior Placements
therapy, remedial education, and
monitoring of the need for pharmacotherapy.
Range
Oto 15
Oto 21
Oto 10
Oto 3
1 to 28
The psychiatric problems of the C'i'T youth include both internalizing (e.g., anxiety, depression
and self-harm behavior) and externalizing (e.g., attentional, impulsive and aggressive behaviors)
problems. Many clients exhibit a combmation of disorders across these broad spectmms. On average,
CTF clients have two major diagnoses (on Axis 1 of the DSM IV)and many of the diagnoses are
characterized bv complicating feamres (e.g., psychotic features associated with a diagnosis of Bipolar
Disorder).
I
The combined figure is an undercount, as counts of prior juvenile detentions are not currently available.
Starlight Summarj- of Program
KLD v.().5/06/05
3 of 5
Types of Disorders (Percent Clients with a Diagnoses)
Most Prevalent Diagnoses
100
90
80
68%
60%
70
Bipolar Disorder
30%
Post Traumatic Stress
29%
Other Mood Disorders
25%
Major Depression
23%
60
50
40
30
12%
20
Att-Def Hyperactivity
22%
Conduct Disorder
19%
Oppositional Defiant
15%
Intermittent Explosive
13%
10
0
Internalizing
Externalizing
Other
Disorders
Disorders
Disorders
Schizoaffective
9%
Schizophrenia
3%
As can be seen in the graph below, Starlight clients have DSM Axis V Global^Assessment of
\hmctionmg(GAP)scores ranging frem 20 to 62 on a 0 to 100 point rating scale, where 100 is optimal
functioning. Tire average GAF score is 36.4, median is 35.0, and the standard deviadon is 8.75 (modest
amount of variadon in physician’s ratings of funedoning).'i'wenty-five percent(25%) of clients have a
GAF score of below 30 upon enrollment.
100
Interpreting GAF Scores
51-60: Reflects moderate difficulties in social or school
funedoning with symptoms not apparent at aU times
or in all areas.
High = 62
Average = 36.4
Low = 20
0
41 -50: Reflects serious impairments in social or school
functioning (e.g., frequent aggressive or antisocial
behavior, suicidal preoccupation).
31-40: Reflects major impairments in several areas
(e.g., persistent aggression without clear
instigation, markedly withdrawn and isolated,
suicide attempts).
Below 30: Serious impairment in almost aU areas (e.g.,
stays in bed all day, severe impairment in reality
testing, communications sometimes incoherent).
Youth Outcomes
Hffecting outreach, family building, and transition planning is always challenging with a high-end
sendee population. Many families are ill-equipped and need much help to receive and maintain troubled
youth in the home. Poor and mentally disturbed young adults struggle with a shortage of safe, low-cost
housing in the Bay Area. Fiducaticmal options are often limited and ongoing support may be needed to
help youth stay focused and on track with educational or vocational endeavors. Cultural competency
implies wc help youth and families with these kinds of everyday life challenges. For all of the above
reasons, permanency or emancipation planning is a major focus of Starlight staff attention and effort.
Starlight Sumniar\- of Program
K1.D v.05/06/05
4of5
One measure of mental health
Increase in Functioning
funcaoning is the change in CjAF
100
scores from admission to
90
discharge. On average, the CrF
youth show a 5.14 gain in their
rating, which is statistically
significant (p <.005)improvement
of modest si2e (that is, clients
move up one scale level on the
description of the GAF found on
the previous page).
80
70
60
50
41.5
36.4
40
30
20
10
0
GAF at Placement
GAF at Discharge
/Vnothcr indicator of
treatment impact is tlic
ability of clients to
transition to a lower level
Placement at Discharge(As Percent of All Discharged Clients)
60.0%
of care. As can be seen
from the chart at right,
over half of youth (64.5%)
are able to step-down to
their family home, foster
family, or a lower level
group home.
Along with the
increasing numbers of
youth admitted from
juvenile probation, we have
48.4%
50.0%
40.0%
29.0%
30.0%
20.0%
16.1%
10.0%
6.5%
seen an increase in
0.0%
discharges back to juvenile
Hospital/Adult
Juvenile Hall
Home/Family
Group Home
hall, usually related to
IMD
significant violence and
aggression. Currently, we
are meeting tins challenge by implementing a restoradve jusdee component to the treatment program.
In summaty^, Starlight remains an intensive, muldfaceted community mental healdr treatment
program for die most seriously emotionally dismrbed youth in California. The program is effeedve in
stabihzing and reuniting youth with their families in shorter periods of dme and with greater frequency
than other previous mental health and social sendee programs. Tlnough the Starlight Community Services
program, Starlight is able to ensure condnued stabiHzadon of these youth in their homes,school and
communit^^
Starlight Summary- of Program
Kl.D v.05/06/().5
5 of5
Document
Demographic of individuals served and referred for Community Treatment Facility (CTF) placement by different public agencies
Initiative
Collection
James T. Beall, Jr.
Content Type
Report
Resource Type
Document
Date
05/06/2005
Language
English
City
San Jose
Rights
No Copyright: http://rightsstatements.org/vocab/NoC-US/1.0/